Consent For Treatment Of A Minor Without Parent Form
Consent For Treatment Of A Minor Without Parent Form - I authorize the following individual, who is a person over 18. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. I have the legal right to consent for medical treatment for this child (patient). By law, any child under the age of 18 years old cannot be seen by a doctor.
I have the legal right to consent for medical treatment for this child (patient). By law, any child under the age of 18 years old cannot be seen by a doctor. I authorize the following individual, who is a person over 18. It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form.
I authorize the following individual, who is a person over 18. I have the legal right to consent for medical treatment for this child (patient). Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. By law, any child under the age of 18 years old cannot be seen by a doctor. It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of.

Consent To Treat A Minor Without Parent Form Ohio 2022 Printable
I authorize the following individual, who is a person over 18. It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. By law, any child under the age of 18 years old cannot be seen by a doctor. Be seen for follow up appointments without a parent/legal.
Basic Printable Medical Consent Form For Minor Printable Form
I have the legal right to consent for medical treatment for this child (patient). I authorize the following individual, who is a person over 18. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. By law, any child under the age of 18 years old cannot be seen.
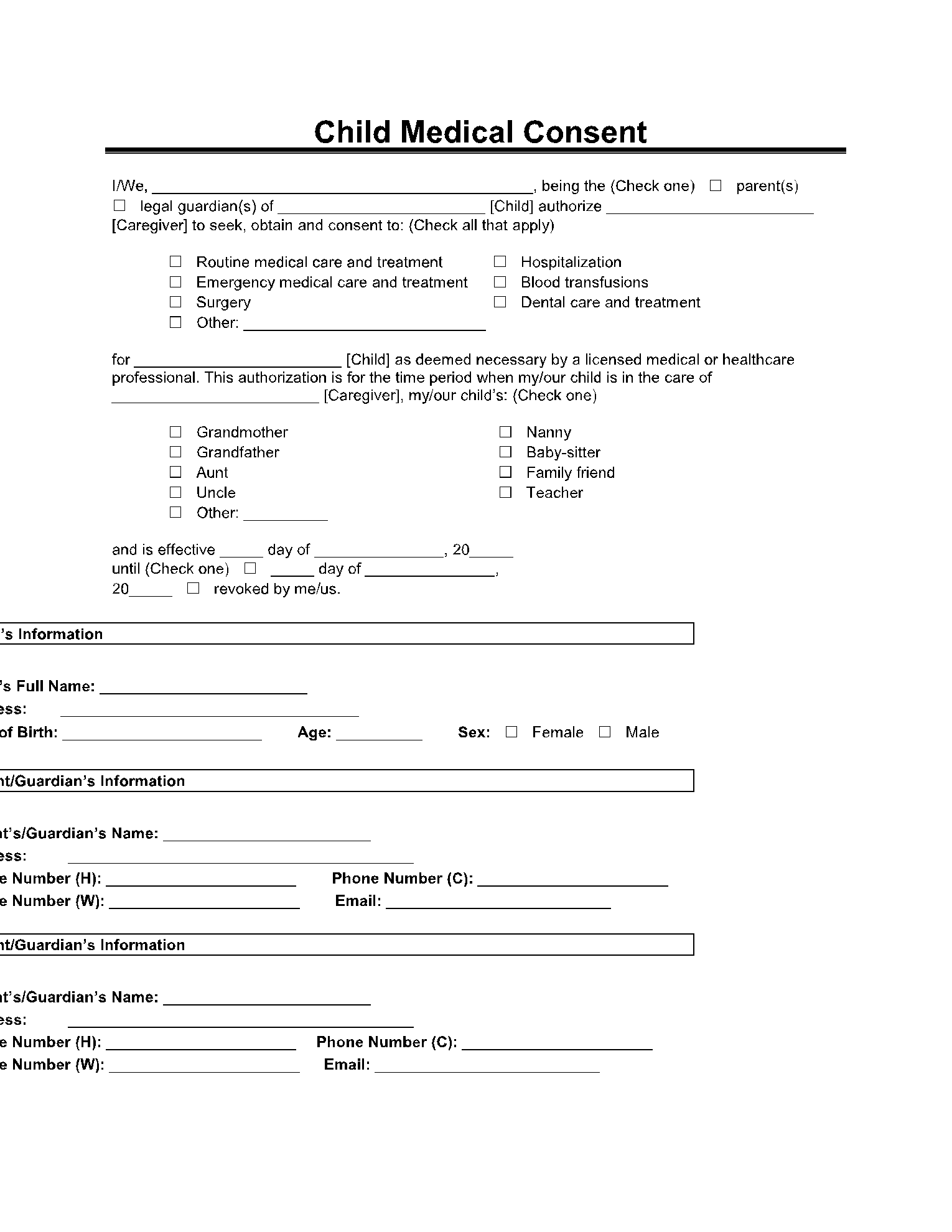
Child Medical Consent Form ⇒ Treatment Permission for Minors
Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. By law, any child under the age of 18 years old cannot be seen by a doctor. I have the legal right to consent for medical treatment for this child (patient). It is intended that this authorization relieve the.

Consent to Treat Minor Children Download the free Printable Basic Blank
It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. I have the legal right to consent for medical treatment for this child (patient). I authorize.
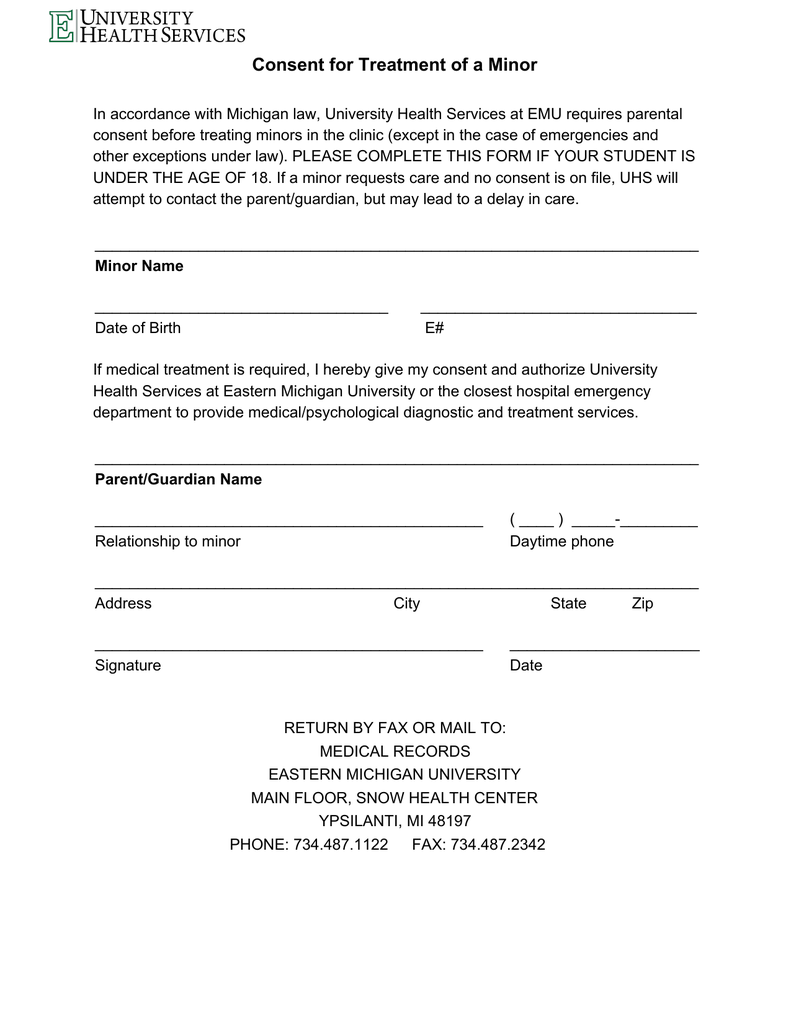
Consent for Treatment of a Minor
I authorize the following individual, who is a person over 18. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. I have the legal right to consent for medical treatment for this child (patient). It is intended that this authorization relieve the physician, dentist, or other person rendering.
Parent Consent Form For Medical Treatment Free Printable Documents
By law, any child under the age of 18 years old cannot be seen by a doctor. I authorize the following individual, who is a person over 18. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. I have the legal right to consent for medical treatment for.
Medical Authorization Form For Children Images Medical Free
I authorize the following individual, who is a person over 18. I have the legal right to consent for medical treatment for this child (patient). It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. Be seen for follow up appointments without a parent/legal guardian only if.
FREE 9+ Sample Medical Consent Forms in PDF MS Word
Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. I have the legal right to consent for medical treatment for this child (patient). I authorize the following individual, who is a person over 18. It is intended that this authorization relieve the physician, dentist, or other person rendering.
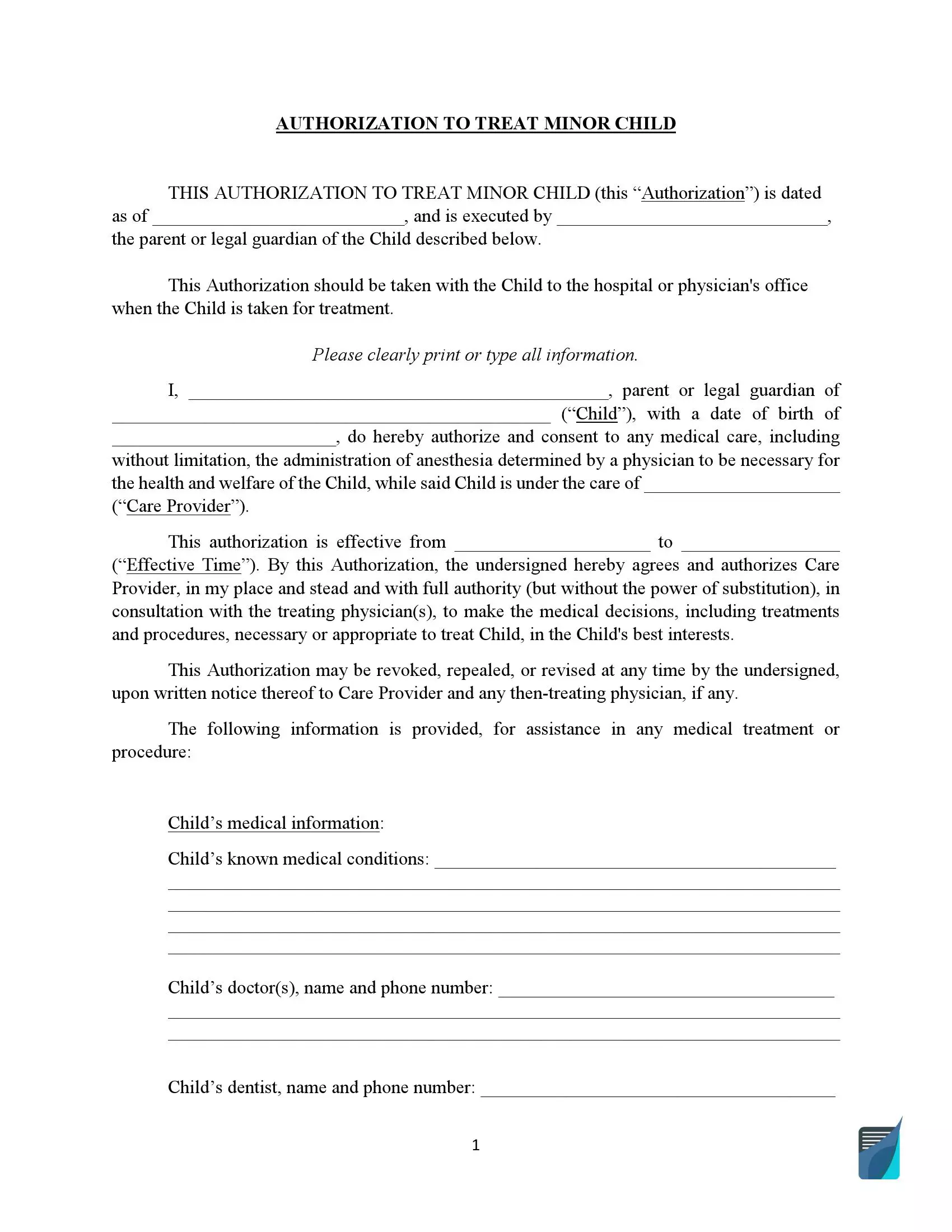
Free Medical Consent for the Treatment of a Minor PDF
It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. I authorize the following individual, who is a person over 18. By law, any child under the age of 18 years old cannot be seen by a doctor. I have the legal right to consent for medical.
Printable Medical Consent Form for Minor While Parents Are Away
I authorize the following individual, who is a person over 18. Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. By law, any child under the age of 18 years old cannot be seen by a doctor. It is intended that this authorization relieve the physician, dentist, or.
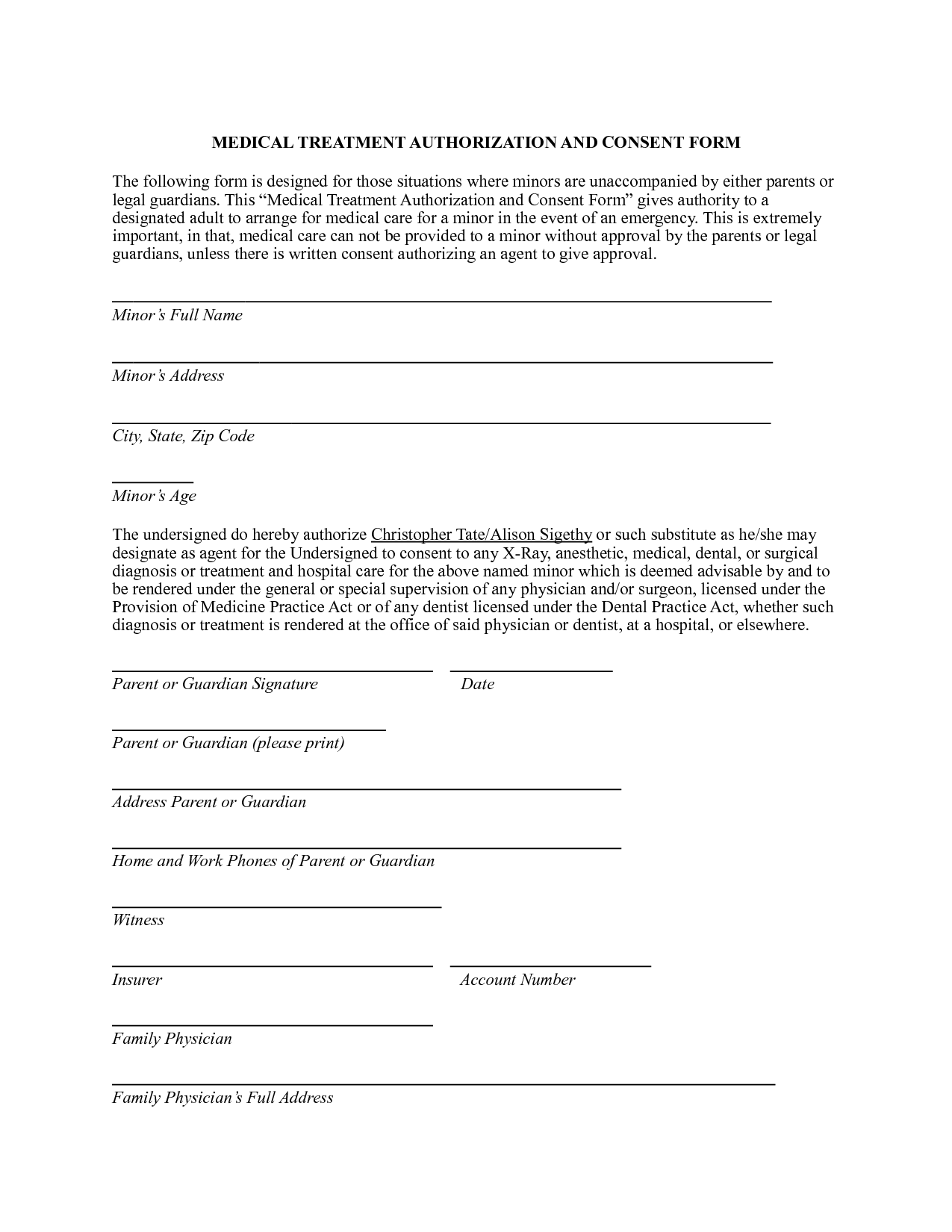
By Law, Any Child Under The Age Of 18 Years Old Cannot Be Seen By A Doctor.
Be seen for follow up appointments without a parent/legal guardian only if parent/legal guardian fills out and signs this consent form. I have the legal right to consent for medical treatment for this child (patient). It is intended that this authorization relieve the physician, dentist, or other person rendering care from any liability resulting from the inability of. I authorize the following individual, who is a person over 18.